
This horror story involves a nurse practitioner led practice in North Carolina. It started out like so many other clinics, an excellent nurse practitioner moves to an underserved area and opens her own clinic. Unfortunately, nurse practitioners in the state of North Carolina (supervision/scope of practice requirements) are required to have a supervising physician and do not have independent prescribing or diagnostic authority. This nurse practitioner was aware of the law and proceeded to find a qualified physician to provide supervision in her new practice.
She found a great board certified family medicine physician to provide supervision and she was on her way to having a vibrant practice. Unfortunately, it’s not enough to just find a supervising physician and hope that they take care of the paperwork involved in registering as your supervising physician. It’s also not enough to trust that the physician supervising your medical services doesn’t already have a dozen other nps that he/she is providing the same services to.
I wish this story had a happy ending but it does not. She hit the ground running, got her practice credentialed with the insurance companies, Medicare, NC Medicaid, selected her billing company and started marketing her new practice with a beautiful new website. After only one year, she was seeing an average of 28 patients each day and even introduced some ancillary services within her practice.
Little did she know, her practice was about to fall apart and her life was going to take a radical turn,
Here are the four issues that shut down a nurse practitioner’s private practice:
- The physician, while well-meaning, was also supervising 11 other nurse practitioners spread out across 3 counties. It was ruled that he could not sufficiently meet the supervision standards as he was rarely available to the nurse practitioner. It’s important to consider to recognize the distinction between a supervising physician in title only and one that is actually involved in your practice.
- The local billing company (that came with excellent recommendations) failed to submit claims properly. While each state has their own definition of what supervision entails, the federal government trumps any local laws when it comes to billing. You’re required to submit claims under the nurse practitioner for any Medicare new patients or established patients presenting with new problems. One can argue that the billing company was aware of this provision(they certainly should be) and that they simply billed all claims under the supervising physician because of the 15% reduction in payment for NPs when billing under their own Medicare number. The whole case against the NP might not have ever been brought up if a patient hadn’t complained about fraudulent billing because an EOB showed a physician’s name that she had never met or heard of.
- If the supervision of too many NPs wasn’t enough, the physician also had disciplinary action against him which all but eliminated his prescribing authority. Nurse practitioners in NC do not have independent prescribing authority to it’s important to verify that your physician doesn’t have any current or pending lawsuits which limit his/her prescribing authority.
- Finally, the NP was told that she would be covered under her supervising physician’s malpractice policy which was never done. It is true that you can be a rider on your supervising physician’s malpractice policy but they have to submit the paperwork and pay the fees to make this happen. Their failure to do so isn’t just their problem, it could come back to bite you in the butt like it did with this NP. We always recommendhaving your own policy to prevent issues down the road when your supervising physician forgets to renew or decides unilaterally that it’s not worth the extra money to cover you.
At the end of the day, the nurse practitioner was fined hundreds of thousands of dollars under the false claims act, forced to shut down her practice and now has a restricted license in the state of NC. You may say that this is a really rare occurrence but it’s happening a lot more than you think. Do your due diligence when starting your practice and take steps to ensure this scenario doesn’t replay in your life. It’s NOT worth it!!
For assistance with starting your np private practice or help with insurance credentialing and contracting, visit our NP Credentialing Services page here.
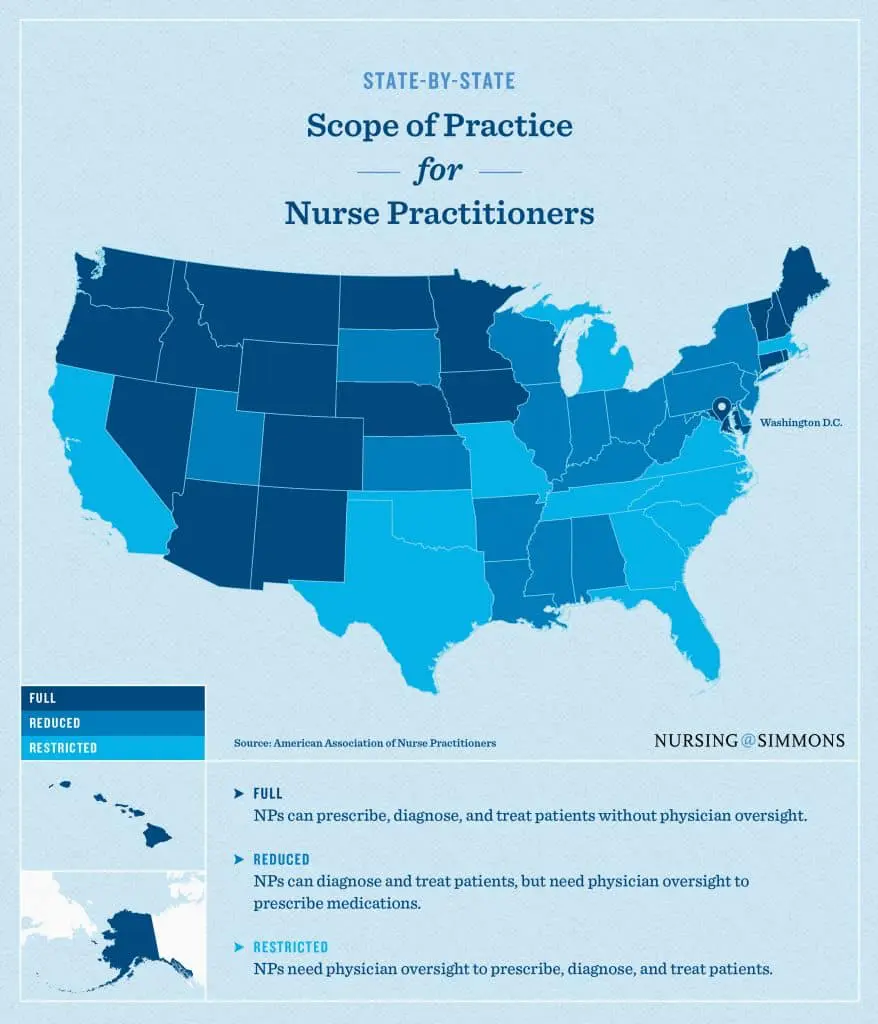
Does my state provide full practice authority to nurse practitioners?
Understanding Practice Status of Nurse Practitioners
Scope of practice guidelines for advanced nursing professions vary by state as indicated above. As of 2022, there are now 33 states(& DC) that allow nurse practitioners full practice authority (without physician oversight). However, some of these states still limit prescribing authority for nurse practitioners with only 24 having full prescribing and practice authority. The Kaiser Family Foundation has a very helpful grid that can be found here “full practice” (Kaiser Family Foundation)
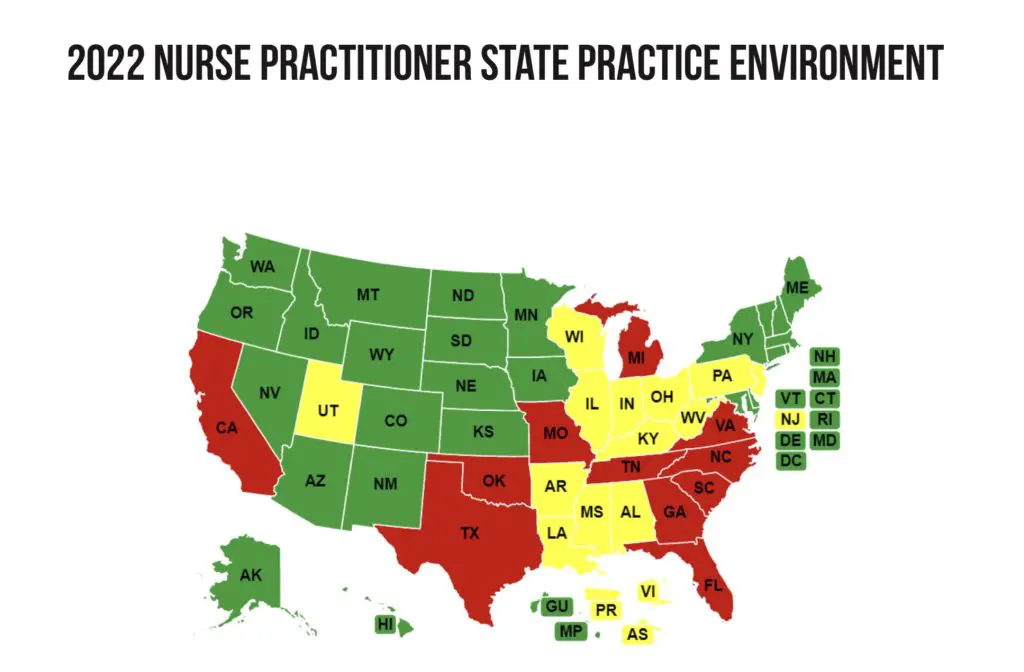

As of 2010, full practice status became the recommended model by the Institute of Medicine and the National Council for State Boards of Nursing. However, not all states are on board with the measure. As mentioned above, there are still 18 states that require a collaboration agreement and and 27 states that restrict prescribing authority.
These practice guidelines do change slightly depending on location and whether or not you are in a federally designated underserved community, NPs must have either a signed collaboration agreement with a physician or direct oversight from a physician. Not all states require the physician to be physically present, be in the same building or even have limits on how many NPs a physician can supervise(crazy right) but your collaborating physician should always be available by phone or email.
Nurse practitioner practice authority defined
1. Full Practice Authority
State practice and licensure laws permit all NPs to evaluate patients; diagnose, order and interpret diagnostic tests; and initiate and manage treatments, including prescribing medications and controlled substances, under the exclusive licensure authority of the state board of nursing.
2. Reduced Practice Authority
State practice and licensure laws reduce the ability of NPs to engage in at least one element of NP practice. State law requires a career-long regulated collaborative agreement with another health provider in order for the NP to provide patient care, or it limits the setting of one or more elements of NP practice.
3. Restricted Practice
State practice and licensure laws restrict the ability of NPs to engage in at least one element of NP practice. State law requires career-long supervision, delegation or team management by another health provider in order for the NP to provide patient care.
NP Indepedence is gaining steam
When we initially wrote this article in 2018, there were only 22 states with full practice authority. In four years, we have seen that number increase significantly with 11 more states signing legislation allowing full practice authority. In addition to these 11 new states, there are bills being worked on currently in numerous other states.
Within the next two years, it is our expectation that there will be 4-5 more states granting full practice authority.
Stay Involved & Stay compliant
As the legislative process continues to proceed, it is vital that as a nurse practitioner, you stay informed about what’s happening in your state. These laws have a dramatic impact on how you practice and it’s on you to get involved and let your voice be heard.
NP Resources:
What does the future hold for nurse practitioner’s independence
Health care leaders across the board agree that we need more conversations addressing the use of NPs as independent practitioners. The physician shortage isn’t going away and NPs are the best solution we have to this problem. Both sides concur that the role of nurse practitioners is vital to the health and delivery of medical care in this nation. Unfortunately, neither can agree on the best way to achieve this goal.
It is obvious that COVID-19 has had a significant role in advancing these conversations. The problem will only continue to compound so our hope is that states will recognize the shortage we are facing and act.
DISCLAIMER: The material contained in this is offered as information only and not as practice, financial, accounting, legal or other professional advice. Correspondents must contact their own professional advisors for such advice.
Updated: 9/1/2022